

Are non-English-talking patients found as immediately in the unexpected emergency section (ED) as English-talking sufferers? If not, is this gap confined to particular non-English languages, or is it consistent across all non-English languages? Is this gap steady on weekdays? Is it additional pronounced on weekends?
It would be almost not possible for a medical or fiscal operations staff in your average emergency department (ED) to answer these inquiries promptly and properly without having the proper facts. What is more, until an personal has an analytical track record, it would be extremely tricky for them to know the place to start off with info exploration. Still these sorts of questions are critically vital and pertinent to being familiar with wellbeing disparities and finally, health fairness.
The COVID-19 pandemic surfaced longstanding social and racial inequities, and COVID’s disproportionate influence on folks from some racial and ethnic groups offered a obvious instance of enduring health disparities throughout the state. Efforts at the federal, condition and area levels are properly underway to start out to mitigate these disparities, such as bettering info transparency and bettering the equity of treatment sent during the wellbeing treatment continuum.
Just one case in point of these an work is at the Department of Crisis Medicine at the University of Michigan Health care School, where by Dr. Christopher Fung, MD, led the advancement of an EHR-derived wellness equity dashboard to allow for the exploration of disparities in ED treatment. We just lately spoke with Dr. Fung about the dashboard and how improved access to knowledge and metrics enables exploration and identification of health disparities that could need even further investigation.
Solutions have been edited for clarity.
Can you describe the intervention to develop a dashboard on disparities in the ED?
As an analytics person, I treatment about amassing the right data in purchase to make knowledge-knowledgeable selections. So commonly, developing a data dashboard like this is practical for two matters: course of action tracking and facts exploration. With course of action monitoring, we’re conversing about tracking a precise process more than time utilizing a metric you know quite effectively (i.e. the range of sufferers witnessed per hour) whereas information exploration is a lot more about asking issues of data, normally with a hypothesis now partly shaped or particular person observations that you’d like to take a look at further more. For case in point, you could possibly query if there are variances in how speedily suffering drugs are presented to sufferers of a distinct race, or dissimilarities in the time it requires to see a health care provider relying on your race. Without anything like a dashboard that permits you to slice and dice facts, it is extremely tricky to check out these wellness disparities to correctly challenge a speculation. For this venture in particular, we leaned far more in the direction of the knowledge exploration side of matters but the dashboard is unquestionably helpful for procedure monitoring as well.
The gain of performing with ED details, unlike other pieces of the medical center other than maybe the working place (OR), is that all of our metrics are common and effectively-validated simply because in the end, EDs require to be as efficient as probable. Most EDs in the place are already meticulously tracking factors like waiting around room time, how prolonged it takes for the physician to see a affected person, how lengthy it requires to get pain prescription drugs and how numerous CT scans or X-rays are requested. Even so, it is unusual that this info is stratified by groups that have the opportunity to be marginalized in their treatment for instance, race, ethnicity, sexual orientation, gender identity, language, faith, age, and excess weight, amid other people. Additionally, it is uncommon that such info is available to people outside scientific and economical functions, these as resident physicians or other trainees.
What led you to take on this work? What job did resident physicians engage in in this project and how has it been valuable for them?
Our goal with this undertaking was to acquire a knowledge dashboard that would give resident doctors with all set access to ED information to aid exploratory investigation on disparities in ED individual treatment as section of an existing high quality enhancement (QI) method. Resident physicians in EDs across the nation participate in a important job in affected individual treatment nonetheless numerous of them have restricted obtain to suitable facts and confined options to interact in removing wellbeing treatment disparities. Not only is the essential knowledge normally not out there to inhabitants, but it is also challenging for them to realize and interact with the information to get the success they are right after.
The EHR-derived wellness equity dashboard, which went live in September 2021, is specifically helpful for citizens as they perform on the QI projects they are tasked with to strengthen wellness fairness challenges. The dashboard presents a unique standpoint enabling people to visualize details having said that they want to uncover or take a look at disparities, get started to comprehend root will cause, acquire interventions and measure their impression.
Our original eyesight was that everybody in the ED would have accessibility to this dashboard and in particular, resident doctors could do the job with their mentors on QI tasks. The reality is that inhabitants are exceptionally occupied lots of of them perform 60-80 hrs and whilst some are extremely investigate-pushed and have interacted with the dashboard, the uptake has been slower than we expected. That reported, we just rolled this out in September 2021 and new procedures and workflows consider time to rollout so we’ll see what the use seems like as we go ahead.
How is the dashboard becoming utilized by scientific team?
A great deal of individuals are employing the dashboard but there are a large amount of advanced views and buttons, which can be a minimal too much to handle. There is a variation amongst something posted for mass consumption, like what you may come across on The New York Times’ “The Upshot” or FiveThirtyEight, the place it’s extra facts-driven journalism with a very simple visualization, than a strong information dashboard like ours. As you begin including interactivity to a dashboard, it can develop into a lot more and additional overwhelming with every single button you can simply click or solution you can alter. So that’s a problem for us to prevail over receiving users of the dashboard to interact with it but not in a way which is frustrating to them or confuses the picture extra.
My general perception is that individuals are a lot far more willing to accept info journalism than they have been just a number of a long time back every media firm is carrying out that now. The common public is finding far more snug with data being introduced this way and the very same issue is taking place in well being care with these types of dashboards and data visualizations.
What classes have you acquired due to the fact utilizing? Did you discover a little something sudden?
Further than the usability obstacle I described, I did not realize how tricky it was for leadership to get facts out of the Byzantine process that is an digital health care document. Given that placing the dashboard out there, I have swiftly understood how previously inaccessible this data was. Before I designed the dashboard, the aged way to get that info was to send out a bunch of e-mails that finally finished up with an analyst running static studies. Now, it’s a great deal simpler to send somebody a url to the dashboard and they can test for by themselves.
Nevertheless, it will get a minimal bit into the weeds when you insert state-of-the-art functions like evaluating two groups towards each and every other for some metric that can turn into a minimal mind-boggling to individuals. So that’s form of my ‘side job’ as a data scientist making the dashboard additional usable for folks other than just myself.
What are your upcoming designs for the dashboard? What updates have you made to the dashboard? What is the status of some of the ‘future directions’ stated in the review?
My main process for this line of investigation is working with knowledge to drive some of our DEI and fairness initiatives. Precisely, encouraging extra use of the dashboard amongst the trainees – the two resident doctors and pupils. They are normally tasked with coming up with wellbeing care fairness QI tasks and there is a wealth of facts they can use to justify the job they’re undertaking which is essential due to the fact most tasks call for purchase-in from nursing team, administrative personnel, and many others. Tasks also demands money, so it is important to back up QI venture requests with difficult information. I want to make the trainees’ interactions with the dashboard – and information in common – easy more than enough so that somebody devoid of an analytical qualifications can do it. They need to have to be equipped to generate the query and then go to the details for a extra in-depth evaluation to develop a rationale for their QI tasks, or to come up with new QI initiatives.
In terms of upcoming instructions, really much just about every ED in the region has this variety of information and facts previously these facts sets we’re using are not that unusual. They are all live and they’re all all set for analytics they just want to be overlaid with some things that might lead to overall health care inequalities like age, race, gender, etcetera. So the for a longer period time period hard work is to scale you can scale throughout a more substantial health care method or even unrelated EDs because every person has this info now you just will need the system to set it alongside one another in a dashboard.
What other health and fitness fairness perform are you endeavor or organizing to undertake? How can well being IT fuel people attempts?
One particular of the items I’m intrigued in checking out is how the triage process biases treatment in the ED. Most men and women really don’t know how influential those people notes are they seriously affect how swiftly you are witnessed by a physician. Quite often that piece of documentation is the only piece that is concluded in your first day at the clinic, so absolutely everyone is examining this 1 triage be aware when you are in the ED. If that notice has inaccurate data or it is biased, that influences your treatment. For illustration, if you show up at the ED in pain but you glance fine, the note will mirror that and there may be an assumption that you never will need to be viewed as urgently. Right or erroneous, those people statements or notes are biasing and they impact extra than just time they also influence no matter whether or not you get suffering prescription drugs, get a CT scan, etcetera. So the language that we use in individuals notes is probably biasing and that’s in which I’m starting up a new line of study dissecting the language we use in triage notes and how that influences treatment down the highway. It is possible we are biasing treatment throughout language or race even if that is not at all our intention for case in point, health professionals have a tendency to describe females as “hysterical” and that has a biasing outcome on what suppliers think of that client, prior to they even go in the space and meet up with the affected individual. One more element is designing interventions to cut down that.
The purpose a dashboard could play in one thing like that is running an algorithm that analyzes the text of the notes primarily based on a language disparity rating, to decide whether or not that language could result in disparities in treatment. One thing like this would be handy to nurses, providers and many others so they can better recognize how the language in notes can be biasing and eventually, attract a clearer line between language and results.
What is some thing that we did not address about this challenge that we need to have?
We’ve collected a ton of information and have a dashboard but some thing which is not highlighted in the short article is genuinely the subsequent phase with a venture like this is acquiring leadership purchase-in. In the end, it is definitely tough for any project to attain momentum without leadership fascination. I’m a college member at a substantial tutorial hospital with entry to all kinds of means and individuals who can aid me do issues even then it is very, quite difficult to change a large ship until the captain of the ship is bought in to wherever you need to go.
To find out extra about ONC’s operate to embrace health and fitness equity by structure, visit HealthIT.gov. To discover much more about the University of Michigan’s wellness fairness dashboard, examine the research.

Determine C: Time to 1st agony medicine by race. Most commonly administered ache prescription drugs were determined a priority. Documented administration time is plotted as a survival curve the place administration of agony medicine is the function of interest. Decrease curves suggest larger likelihood of receiving agony treatment.
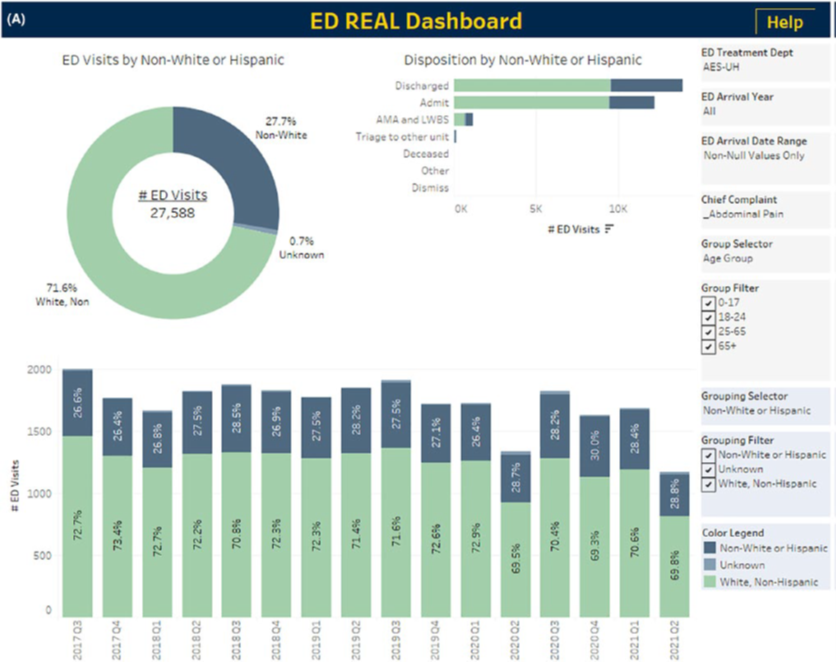
Determine A: Case in point exploratory analyses employing the dashboard for first pain treatment by race and ethnicity in patients presenting with abdominal ache. Authentic, Race, Ethnicity, and Language. All panels are filtered to adult ED visits for abdominal soreness and stratified by the pursuing teams: White and non-Hispanic, non-White or Hispanic, and unknown race/ethnicity. Other selectable filters are at the appropriate of every single panel. (A) Total and quarterly distribution of ED visits by race with disposition. Counts and percentages are displayed for each and every of total visits, quarterly visits, and dispositions.




More Stories
10 simple tactics to tackle anxiety and lift your mood
7 Famous Celebrities Who Weighs 165 Lbs In Kg (74.8 Kg)
Can You Eat Eggs After Tooth Extraction?